Pregnancy
Pregnancy covers the life stage period from conception to birth. Learn about the changes that take place during this time, what to do to stay healthy, and how to help prevent complications during pregnancy.

The Shocking Story of Lina Medina, Who Gave Birth at Age 5

You Can Get Pregnant When You're Already Pregnant

Can you get pregnant after having gonorrhea?
Exercise During Pregnancy

Can a woman get pregnant during her period?

Does diabetes affect fertility?

Hormone Imbalances and Infertility

What Do Babies See Before Birth?

Guide to Being 39 Weeks Pregnant

Guide to Being 28 Weeks Pregnant

C-sections Can Affect a Baby's Immune System

Quick Tips: Pedicures and Labor

How a Baby Experiences Labor and Delivery

How to Deal with Swelling After Pregnancy

How does postpartum depression affect infants?

How to Minimize Stretch Marks After Pregnancy

Miscarriage Overview
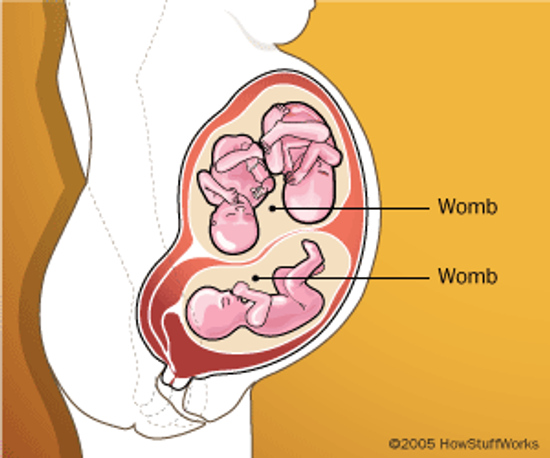
If a Woman Has Two Wombs, Can She Get Pregnant in Both?

A Guide to Pregnancy Complications

Rare Condition Causes New Mom to Lactate Outside Her Breast

What Is the Linea Nigra of Pregnancy?

Is it possible for a pregnant woman to be allergic to the placenta?
Learn More

The world's youngest mother, Lina Medina, gave birth to a healthy baby boy at age 5 in 1939. But how could that happen?
By Dave Roos

An Austrian woman who had just given birth began producing milk in breast tissue located in her vulva.

The dark line that runs down a pregnant woman's belly is completely normal, and it even has a fancy Latin name.
Advertisement

Very little is known about what or how fetuses see. This study shows their vision capabilities are more advanced than previously thought.
By Alia Hoyt

It's extremely rare but not unheard of. So, how does it happen?
By Alia Hoyt

But researchers are working on a method to boost the microbiota of babies born by C-section.

It seems unbelievable that a baby's placenta could cause the mother to break out in a nasty itchy rash, but it happens occasionally. What causes the allergy?
By Alia Hoyt
Advertisement

Pregnancy brings women that lovely glow -- shiny hair, great skin, an aura of happiness. It also brings some not-so-lovely things, like excessive burping and farting. Go ahead, blame the baby! Here's why.

Pregnancy is all about celebrating your body. But is it safe to celebrate it permanently -- with a tattoo? Here's what we know.
By Debra Ronca

There is no hard, scientific evidence proving that a pedicure -- or foot massage – will help induce labor if you've carried full term. Then again, why not try it?

As far as contraceptives go, intrauterine devices (IUDs) are generally the most effective method short of abstinence. But does highly effective mean fool-proof?
Advertisement

When it comes to keeping track of your birth control, Depo-Provera -- administered via injection from your physician every 12 weeks -- seems to eliminate a lot of worry. But how effective is it?

Finding out you have gonorrhea and learning how to treat it can be challenging enough. But you also need to be aware of how this STI could affect your fertility.

Though the evidence is largely anecdotal, there are some simple steps you can take to improve your chances of getting pregnant, including a change in positions.

The miracle of life brings joy to many expecting parents when they welcome a child into the world. But an improperly functioning thyroid gland could make conception a challenge.
Advertisement

Pregnancy myths abound, but one of the most common is that it's impossible to get pregnant while on your period. Why is this idea so off-base, and what does the textbook 28-day cycle have to do with it?

The long, complicated process of labor and deliver is believed to be started by the baby. Learn what a baby experiences during labor and delivery.

When getting pregnant is your goal, it can be extremely frustrating to discover your body is actually working against you. How can imbalanced hormones thwart your attempts, and what can you do to treat the problem?

There was a time when women with diabetes were strongly advised to avoid getting pregnant, though caregivers no longer give that direction. But how does diabetes affect fertility?
Advertisement

Uterine fibroids are extremely common, affecting 20 to 40 percent of women over the age of 35. Can these often benign growths alter your chances of getting pregnant?

It's well-documented that a sedentary lifestyle can have negative effects on your health. But can too much exercise harm your fertility?

Peruvians have eaten maca root for thousands of years, and it's earned a reputation as an aphrodisiac. But can it boost your fertility?

Prescription pain medication can make daily life a lot more tolerable for people suffering from chronic conditions. But could they also rob you of your ability to conceive?
Advertisement

It's no secret that hormones play a major role in both the female and male reproductive systems. But why is progesterone called the hormone of pregnancy?

Milk, the slogan says, does a body good. But when it comes to your fertility, can there be too much of a good thing?